
You’re eating well. Maybe you’ve even cleaned up your diet significantly — less processed food, more vegetables, adequate protein. You’re doing the things.
And you’re still exhausted. Still gaining weight or unable to lose it. Still running on caffeine just to function.
Here’s what most practitioners miss: you can eat plenty of calories and still be energy-depleted at the cellular level.
Not because you’re eating the wrong foods. But because your cells are missing the specific raw materials they need to convert that food into usable energy.
This is the micronutrient-metabolism connection — and it’s one of the most overlooked drivers of stubborn fatigue, weight resistance, and metabolic dysfunction.
Why Eating Less Doesn’t Fix a Nutrient Problem
Your mitochondria are the organelles inside every cell that produce ATP — the actual currency of cellular energy. Everything you experience as “energy” comes from mitochondrial ATP production.
But here’s what the calorie-counting model completely ignores: mitochondrial function depends on specific cofactors to run the electron transport chain.
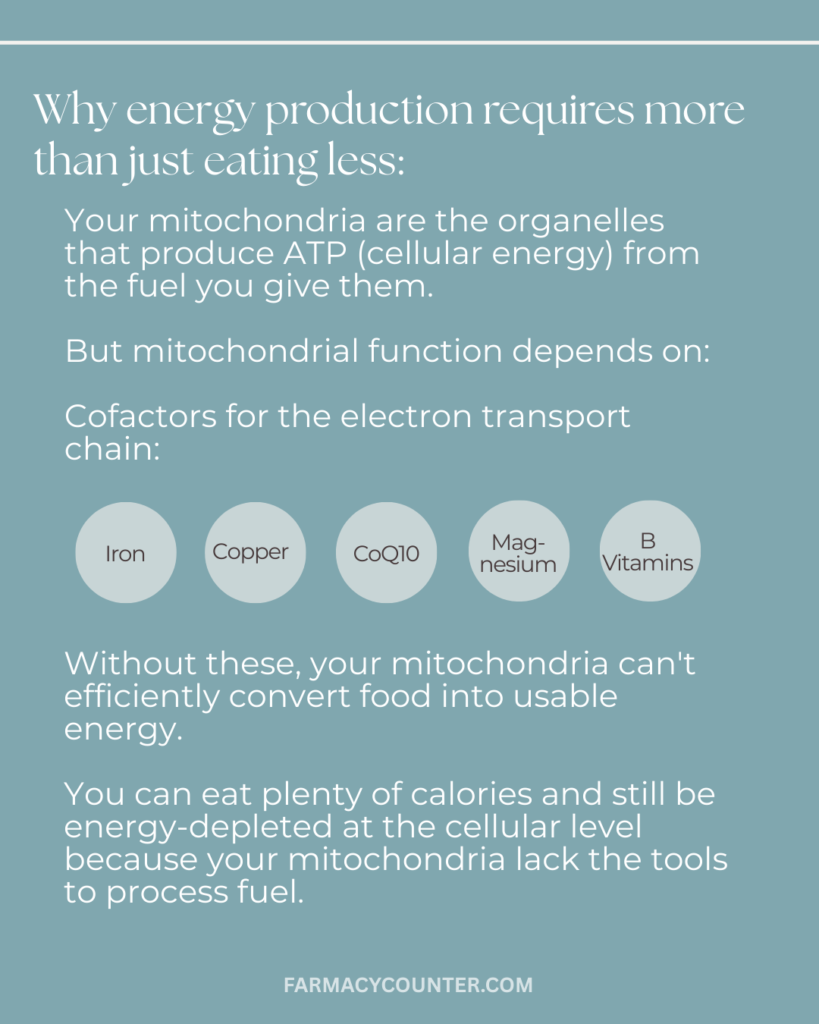
Without adequate iron, copper, CoQ10, magnesium, and B vitamins, your mitochondria cannot efficiently convert food into usable energy — regardless of how many calories you’re consuming or how clean your diet is.
This is why two people can eat identical diets and have completely different energy levels and metabolic responses. One has the micronutrient status to actually run the machinery. The other doesn’t.
And when you restrict calories further in an attempt to lose weight, you often make this worse — eating less means taking in even fewer of the micronutrients your metabolism depends on.
The 5 Micronutrients Dr. Ryan Tests in Every Complex Metabolic Case

1. Magnesium
Optimal level: RBC magnesium above 5.5 mg/dL (not serum magnesium — that number is almost always “normal” even when you’re depleted)
Magnesium is a cofactor in over 300 enzymatic reactions in the body. It’s required for ATP synthesis, glucose metabolism, and insulin signaling. When magnesium is low, virtually every metabolic process slows down.
Deficiency symptoms include muscle cramps, sleep disruption, anxiety, and insulin resistance — all of which are commonly attributed to other causes while the underlying magnesium depletion goes untested.
The critical detail: standard serum magnesium tests miss deficiency in the majority of cases. RBC magnesium measures what’s actually inside your cells, where it matters.
2. Vitamin D
Optimal level: above 40 ng/mL
Vitamin D functions more like a hormone than a vitamin, with receptors in virtually every tissue in the body. It directly regulates insulin sensitivity, modulates immune function and inflammation, and affects mitochondrial function at the cellular level.
Deficiency drives insulin resistance, increases inflammatory markers, and contributes to the kind of deep fatigue that sleep doesn’t fix. Most people who are tested are told their levels are “fine” at 25-30 ng/mL — but optimal metabolic function requires levels above 40.
3. Zinc
Optimal level: above 90 µg/dL
Zinc is required for thyroid hormone receptor function — meaning even if your thyroid is producing adequate hormone, low zinc can prevent your cells from responding to it properly. It’s also essential for insulin signaling and tissue repair.
Deficiency manifests as poor wound healing, hair loss, immune dysfunction, and impaired taste or smell. In the context of metabolic dysfunction, zinc deficiency is particularly insidious because it can make thyroid labs look normal while thyroid function is still impaired at the cellular level.
4. Iron (Ferritin)
Optimal level: ferritin above 50 ng/mL
Iron is required for thyroid hormone production, essential for mitochondrial ATP production, and needed for oxygen transport to every cell in your body. Without adequate iron, your cells literally cannot produce energy efficiently.
Ferritin — the storage form of iron — is the marker that matters most. Levels between 12-30 ng/mL are technically “in range” by most lab standards, but functionally insufficient for optimal metabolism. Patients with ferritin in the teens or low twenties often experience profound fatigue, hair loss, cold intolerance, and complete exercise intolerance — and are told their iron is normal.
This is one of the most common and most missed drivers of metabolic dysfunction in driven women who have been restricting calories for years.
5. B Vitamins (especially B12, folate, and B6)
Optimal level: B12 above 500 pg/mL
B vitamins are required for methylation, neurotransmitter production, and critically — the Krebs cycle, which is the metabolic pathway your cells use to generate ATP from fuel. Without adequate B vitamins, the entire energy production process stalls.
B12 deficiency in particular causes fatigue, brain fog, and mood dysregulation that is frequently misattributed to depression or burnout. Standard lab reference ranges flag deficiency at levels below 200-300 pg/mL — but neurological and metabolic symptoms commonly appear at levels below 500.
Hormonal birth control depletes B vitamins significantly, as does chronic stress, alcohol, and a diet low in animal products.
Why “Just Take a Multivitamin” Doesn’t Work
Identifying these deficiencies is only half the equation. The other half is correcting them properly.
Generic supplementation often misses the mark because:
- Form matters. Magnesium oxide has poor absorption; magnesium glycinate or malate are far better utilized. Cyanocobalamin (the cheap B12) is poorly converted in people with MTHFR variants; methylcobalamin is more bioavailable.
- Dose matters. Therapeutic repletion of a true deficiency requires higher doses than a standard multivitamin provides — and for longer than most people realize.
- Interactions matter. Iron and zinc compete for absorption. Vitamin D requires cofactors (vitamin K2, magnesium) to be properly utilized.
- Testing first matters. Supplementing without knowing your actual levels means you might be adding nutrients you don’t need while missing the ones you do.
The functional medicine approach is to test, not guess — identify what’s actually depleted, replete to optimal ranges (not just “in range”), and retest to confirm.
The Labs That Actually Reveal Micronutrient Status
Standard annual bloodwork almost never includes the right tests. The markers that reveal true micronutrient status:
- RBC magnesium (not serum)
- Ferritin, serum iron, TIBC, transferrin saturation (complete iron panel)
- Zinc (serum or RBC)
- Vitamin D 25-OH
- Methylmalonic acid + homocysteine (functional B12/folate status — far more accurate than B12 alone)
These are the tests that show what’s actually happening inside your cells — not just what’s floating in your bloodstream.
What Happens When You Correct the Deficiencies
This is where the results that look “too good to be true” actually come from.
When a patient comes in exhausted, weight-resistant, and convinced their metabolism is permanently broken — and the root cause turns out to be ferritin of 16 and depleted magnesium — correcting those deficiencies can produce dramatic, rapid improvement.
Not because we did anything miraculous. But because we gave the body what it was missing to do its job.
Energy production requires raw materials. When you supply them, the machinery runs.
Find Out What’s Driving Your Metabolic Resistance
Micronutrient deficiencies are just one piece of the metabolic puzzle. Stubborn weight resistance and fatigue typically involve overlapping patterns — nutrient depletion, sleep debt, inflammatory burden, hormonal dysregulation, and more.
The free Weight Resistance Decoder Guide walks you through the four hidden metabolic patterns that drive stubborn weight resistance, including which symptoms point to which pattern and what functional testing actually reveals the root cause.
Your body isn’t failing you. It’s waiting for the right raw materials.





