
If you have ever felt a wave of anxiety arrive seemingly out of nowhere — heart racing, shallow breathing, a sense of dread or hypervigilance that you couldn’t attach to anything specific — and then noticed it ease after you ate something, there is a clinical explanation for that experience that most people have never been offered.
Your blood sugar may have just hit the floor.
Not dramatically. Not dangerously. But low enough to trigger a counter-regulatory stress hormone response — a surge of adrenaline and cortisol designed to pull glucose back up — that produces physiological symptoms that are virtually indistinguishable from anxiety.
This is not a metaphor. It is a mechanism. And it is one of the most underinvestigated contributors to anxiety symptoms in clinical practice today.
What Anxiety Actually Feels Like — and What’s Producing It
When blood sugar drops below a certain threshold, the body treats it as an emergency. The brain is the most glucose-dependent organ in the body, consuming approximately 20% of total glucose supply despite making up only 2% of body weight. When glucose availability drops, the brain activates the hypothalamic-pituitary-adrenal axis and triggers the release of counter-regulatory hormones — primarily adrenaline (epinephrine) and cortisol — to mobilize stored glucose and restore supply.
Adrenaline, in particular, produces a very specific set of physiological effects. It increases heart rate. It raises blood pressure. It causes blood vessels in the periphery to constrict. It triggers rapid, shallow breathing. It heightens alertness and produces a state of hypervigilance — the body scanning for threat, ready to act.
These are also the defining physical symptoms of anxiety.
Racing heart. Tight chest. Shallow breathing. The sense that something is wrong even when nothing identifiable has happened. The inability to settle or concentrate. A generalized dread that arrives without obvious cause and resists logical reassurance.
When blood sugar drops produce an adrenaline surge, the brain experiences that surge as threat — because that is what adrenaline physiologically communicates. The emotional interpretation follows the physiology. The body is in a stress state. The mind looks for a reason.
The Timing Signature That Identifies It
The single most reliable way to distinguish a blood sugar-driven anxiety episode from a psychologically-driven one is timing.
Blood sugar anxiety has a predictable schedule. It is not random. It follows the glucose curve.
Mid-morning, around 10 to 11am, is the most common window. If breakfast was carbohydrate-heavy or was eaten too early, blood sugar may have spiked and then dropped sharply before the morning is half over. By 10 or 11am, the drop is reaching its lowest point. Adrenaline responds. Anxiety arrives. On schedule, every morning, predictably enough that many people have come to think of the mid-morning anxiety as simply how they are.
Before meals — particularly before lunch and dinner — is another reliable window. As blood sugar falls in the hours between meals, some people drop into the threshold that triggers counter-regulatory hormone release before they ever feel conventionally hungry. The anxiety arrives before the hunger does. The meal resolves it, not because eating calms anxiety psychologically, but because glucose is restored and the adrenaline surge subsides.
Upon waking, before eating anything, is a third common pattern. The cortisol awakening response — a natural sharp rise in cortisol in the first 30 to 45 minutes after waking — can drive a glucose release from the liver that then drops before breakfast. Some people wake into this drop already in progress, experiencing morning anxiety, dread, or a low-grade sense of threat before the day has begun.
If your anxiety follows any of these timing patterns — arriving on a schedule, worsening before you eat, easing after you eat — the blood sugar piece warrants investigation.

Why This Gets Missed
There are several reasons this connection is almost never identified in standard care.
The first is that anxiety and blood sugar dysregulation are managed by different specialties and assessed with different tools. Someone presenting with anxiety receives a mental health evaluation. Someone presenting with blood sugar concerns receives a metabolic evaluation. The overlap between the two is rarely investigated.
The second is that standard blood sugar testing does not capture the dynamic. A fasting glucose value taken in the morning reflects blood sugar at rest, under optimal conditions. It says nothing about what blood sugar does at 10:45am, 90 minutes after a carbohydrate-heavy breakfast, when the anxiety arrives. The event that matters is occurring hours before or after the test is run. It is invisible to the snapshot.
The third is that the physiological experience of blood-sugar-driven anxiety is genuinely indistinguishable from psychologically-driven anxiety at the symptom level. Racing heart, shallow breathing, hypervigilance, dread — these feel the same regardless of origin. Without knowing to look for the pattern, there is no obvious reason to question the mental health diagnosis.
The result is that a meaningful number of people are managing blood sugar events with anxiety interventions — therapy, breathing exercises, medication — that address the psychological experience without ever touching the metabolic driver producing it. The interventions can help manage the symptoms. They cannot address the underlying cause.
The Mechanism in Detail: Reactive Hypoglycemia
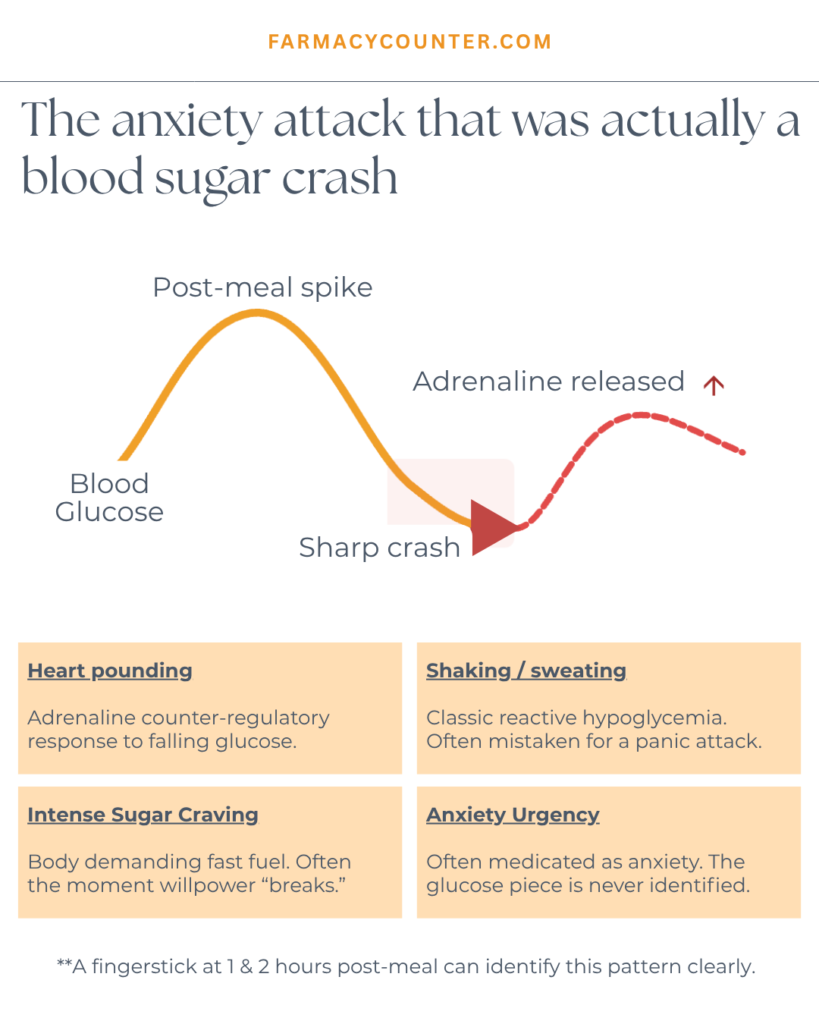
The clinical term for this pattern is reactive hypoglycemia — a drop in blood sugar following a meal that is sharp enough to trigger counter-regulatory hormone release, even when fasting levels look entirely normal.
Here is the sequence in full.
A meal — particularly one high in refined carbohydrates and low in protein and fat — raises blood sugar relatively quickly. The pancreas responds with an insulin release proportional to the perceived glucose load. In someone with early insulin resistance or impaired first-phase insulin response, this insulin release can be excessive relative to the actual glucose level, driving blood sugar down below baseline — sometimes significantly below.
When blood sugar drops into the reactive range — typically below 70mg/dL, though symptomatic responses can occur at higher levels in individuals who are metabolically sensitized — the counter-regulatory response activates. Adrenaline and cortisol are released. Blood sugar begins to recover. But the adrenaline surge has already produced its physiological effects.
The person feels anxious. Their heart is racing. Their breathing is shallow. They are hypervigilant. They may feel shaky or irritable. They may have difficulty concentrating. And then they eat something, the glucose is restored, the adrenaline subsides, and within 20 to 30 minutes the anxiety is gone.
This is a blood sugar event. From beginning to end.

The Cortisol-Anxiety Loop
There is a related but distinct mechanism that operates in people with chronically elevated cortisol — the pattern common in individuals living with sustained stress, inadequate sleep, or HPA axis dysregulation.
Cortisol is a blood sugar hormone. One of its primary jobs is to raise blood glucose by signaling the liver to release stored glucose through gluconeogenesis. When cortisol is chronically elevated, it produces a low-grade but persistent blood sugar elevation that then cycles through the insulin response and downstream drops throughout the day.
Chronically high cortisol also produces anxiety directly — cortisol activates the amygdala and keeps the nervous system in a state of low-grade threat readiness. The blood sugar cycling amplifies this by adding adrenaline surges on top of the cortisol baseline.
The result is a person who is anxious most of the time, with periodic acute spikes that correspond to blood sugar drops, in a context where the entire nervous system is running elevated. Managing the anxiety without addressing the cortisol picture produces incomplete results at best. The cortisol continues to drive both the blood sugar instability and the baseline anxiety simultaneously.
What This Means If This Is Your Pattern
If you recognize the timing signature — anxiety that arrives mid-morning, before meals, or immediately on waking — the following observations are clinically relevant.
Eating protein and fat before or with carbohydrates at every meal significantly buffers the postprandial glucose rise and reduces the depth of the subsequent drop. Protein triggers GLP-1 secretion, which slows gastric emptying and flattens the glucose curve. Fat does the same. A breakfast built around protein and fat rather than carbohydrates alone is often the single most impactful intervention for mid-morning anxiety that has a blood sugar component.
Meal spacing matters. Allowing 4 to 5 hours between meals without snacking is appropriate for metabolically stable individuals, but for someone experiencing reactive hypoglycemia, shorter intervals — eating every 3 to 4 hours — may prevent the drops that trigger the counter-regulatory response.
The cortisol picture needs to be considered alongside the glucose picture. If the anxiety is present not just at the timing windows associated with blood sugar drops but also in the morning before eating and persistently throughout the day, cortisol is likely a significant driver. Addressing the cortisol piece — through stress reduction, sleep optimization, adrenal support, and HPA axis regulation — changes the entire metabolic environment, not just the glucose behavior.
And the testing that actually captures this pattern — fasting insulin, HOMA-IR, and ideally continuous glucose monitoring during the symptomatic windows — provides the data needed to understand what’s happening and build a targeted approach.

Not Saying Anxiety Isn’t Real
To be direct about something important: none of this is an argument that anxiety is not a genuine and sometimes serious clinical condition. It is. And for many people, it has roots that are primarily psychological, neurological, or related to life circumstances that have nothing to do with blood sugar.
What this is is an argument that the metabolic piece is almost never investigated as part of the anxiety picture. And for a meaningful subset of people experiencing anxiety — particularly those who notice it arriving on a schedule, easing after meals, or worsening in the predictable windows described above — the blood sugar connection is not a secondary consideration. It is the primary driver.
When the physiology is addressed, the anxiety often changes. Not because of mindset work or psychological reframing, but because the body is no longer generating the adrenaline surges that the mind has been interpreting as threat.
That is what investigation looks like. And it starts with asking the right questions about timing.
If your anxiety follows a predictable pattern — arriving before meals, mid-morning, or on waking — your cravings and symptom timing may be telling you something specific about what’s driving it. The Cravings Root Cause Quiz identifies whether your pattern is metabolic, hormonal, or stress-driven in two minutes.
Ready to understand the full picture? The Blood Sugar Rhythm masterclass walks through exactly how blood sugar drives energy, mood, and anxiety — and what to do about it.





