
Bloating is a symptom. Not a diagnosis.
That distinction matters more than most people realize, because the way conventional medicine treats bloating — and the way most people approach it on their own — is to treat it as one thing with one solution. Eliminate gluten. Take a probiotic. Try low FODMAP. Avoid dairy.
Sometimes that helps. Often it doesn’t. And when it doesn’t, people assume the problem is them — that their gut is just particularly difficult, particularly sensitive, particularly resistant to improvement.
It isn’t. The problem is that bloating has at least ten physiologically distinct root causes, each with a different mechanism, a different symptom pattern, and a completely different treatment approach. Treating cause number two with a protocol designed for cause number seven doesn’t just fail to help — it can actively make things worse.
This is why the same protocol doesn’t work for everyone. Not because some people’s bodies are more broken than others. Because the mechanisms are different and the interventions need to match.
Here are the ten root causes I assess in clinical practice — and why each one requires a specific approach rather than a generic gut healing protocol.
1. SIBO: Small Intestinal Bacterial Overgrowth
SIBO is one of the most common and most consistently missed drivers of chronic bloating. Bacteria that belong in the colon colonize the small intestine — where they don’t belong — and ferment carbohydrates before your body can absorb them.
The timing pattern is specific: gas and distension typically start 30 to 90 minutes after eating, as bacterial fermentation kicks in on recently consumed food. The bloating often progresses through the day as fermentation accumulates across meals.
Two distinct types of SIBO require completely different treatment protocols. Hydrogen-dominant SIBO involves bacteria that produce hydrogen gas, creating diarrhea-predominant symptoms and rapid fermentation. Methane-dominant SIBO involves archaea that produce methane — which actually slows gut motility — creating constipation-predominant patterns, harder-to-treat overgrowth, and bloating that’s often worse in the morning.
This distinction matters clinically because the treatment that works for hydrogen SIBO can be inadequate or even counterproductive for methane SIBO. And certain probiotics that are commonly recommended for gut health — particularly hydrogen-producing Lactobacillus strains — can worsen hydrogen SIBO by feeding the overgrowth.
SIBO is diagnosed with a breath test measuring hydrogen and methane gas production after a sugar challenge. Up to 60 to 80% of people diagnosed with IBS have SIBO as an underlying driver — most of whom were never tested for it.

2. Low Stomach Acid (Hypochlorhydria)
Low stomach acid is one of the most under-recognized drivers of upper abdominal bloating — and one of the most counterintuitive, because most people assume bloating and reflux mean too much acid, not too little.
When the stomach doesn’t produce adequate hydrochloric acid, food isn’t properly acidified before it moves into the small intestine. Proteins don’t break down efficiently. The pH of the stomach contents doesn’t signal the pyloric valve to open at the right time, so food sits longer than it should. It ferments. Gas accumulates.
The bloating pattern tends to sit in the upper abdomen — that tight, heavy, full feeling that sets in during or shortly after eating. Belching is common. There’s often a sensation of food just sitting there rather than moving through.
Hypochlorhydria affects an estimated 30 to 50% of people over 35, yet is almost never tested in standard GI workups. It’s also one of the setup conditions for SIBO — because stomach acid is one of the primary antimicrobial defenses that prevents bacteria from migrating upstream into the small intestine. When acid is low, that defense drops.
Proton pump inhibitors — among the most prescribed medications in the world — further suppress stomach acid production, which is why people on long-term PPI therapy frequently develop SIBO and worsening bloating despite taking medication designed to reduce discomfort.

3. Impaired Migrating Motor Complex
The migrating motor complex — MMC — is one of the least known but most clinically important mechanisms in gut function. Between meals, approximately every 90 to 120 minutes, the MMC runs a sweeping wave through the small intestine that clears residual food particles, bacteria, and debris downward toward the colon.
Think of it as the gut’s housekeeping cycle. It only runs when you’re not eating — which is why frequent snacking is one of the primary disruptors of MMC function. Every time you eat, the MMC resets and waits until the next fasting window to run.
When the MMC is impaired, bacteria accumulate in the small intestine between meals rather than being swept downward. This creates the exact conditions for SIBO to develop — or to return after treatment, which is why SIBO recurrence is so common in people whose MMC dysfunction hasn’t been addressed.
Chronic stress disrupts MMC function through vagus nerve signaling. Certain medications — particularly opioids and some antidepressants — suppress MMC activity. Previous gut infections that damaged the enteric nervous system can impair MMC function long after the infection resolves. This last mechanism — post-infectious MMC dysfunction — is increasingly recognized as a significant driver of post-infectious IBS.
Restoring MMC function typically requires prokinetic agents — compounds that stimulate the MMC to fire properly — along with meal spacing of at least four to five hours to allow the MMC to complete its cycle.
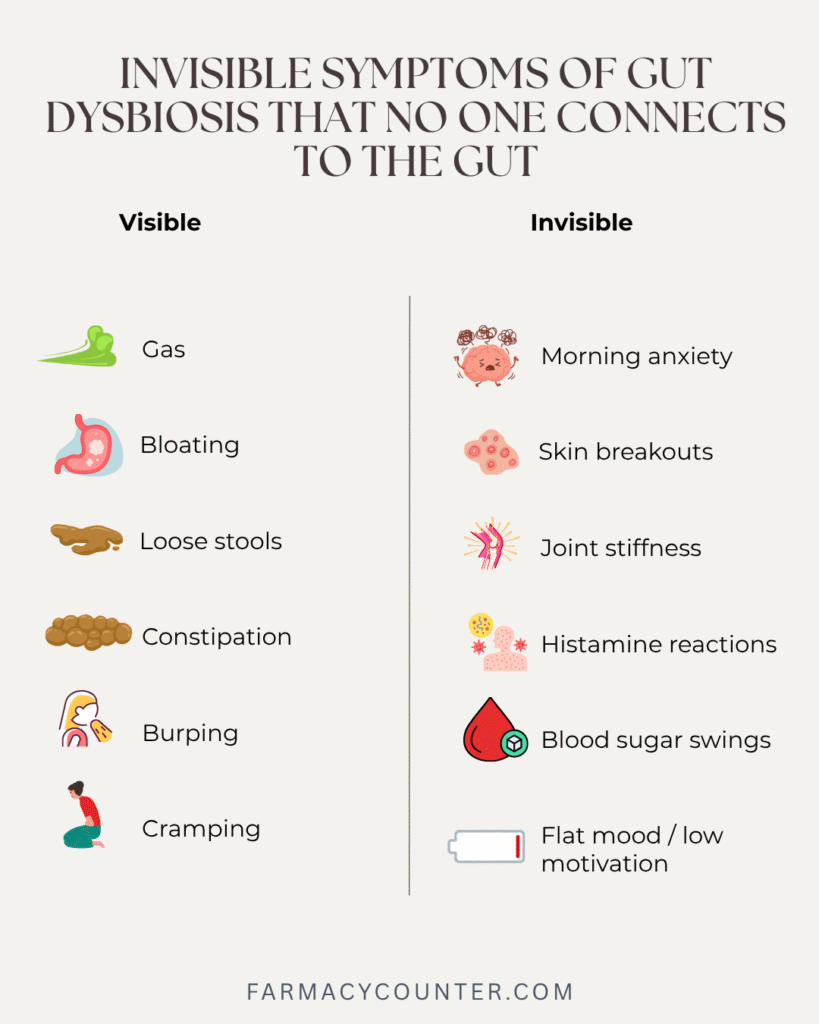
4. Dysbiosis
Dysbiosis — an imbalanced microbial community in the gut — creates bloating through three simultaneous mechanisms: excess fermentation, altered motility, and gut wall inflammation.
When pathogenic or opportunistic bacteria overgrow at the expense of beneficial species, fermentation becomes excessive and imbalanced. Rather than producing the beneficial short-chain fatty acids that healthy bacteria generate, dysbiotic bacteria produce excess gas, inflammatory metabolites, and compounds that damage the gut lining.
Motility changes because gut bacteria directly influence the enteric nervous system — the network of neurons embedded in the gut wall that controls peristalsis. Dysbiosis disrupts the neurotransmitter signaling that coordinates gut movement, creating patterns of sluggish transit, unpredictable bowel movements, and the kind of fermentation buildup that creates progressive bloating through the day.
Gut wall inflammation develops as dysbiotic bacteria produce LPS and other inflammatory compounds that activate immune cells in the intestinal lining. That inflammation further damages the gut wall, reducing digestive enzyme production, impairing nutrient absorption, and creating the conditions for intestinal permeability to develop.
Dysbiosis is diagnosed through comprehensive stool analysis — not a standard stool culture, which only looks for pathogens, but a full GI-MAP or similar test that shows bacterial diversity, opportunistic species, inflammatory markers, and digestive function markers.
5. Intestinal Permeability
Intestinal permeability — leaky gut — creates chronic bloating through immune activation rather than fermentation. When the tight junction proteins that seal the gut lining become compromised, food proteins that should stay in the gut cross into the bloodstream.
The immune system recognizes these food proteins as foreign and mounts antibody responses against them. Those immune responses create gut wall inflammation that drives chronic bloating — inflammation that’s present regardless of what you eat, because it’s being driven by immune activation rather than by a specific food trigger.
This is the mechanism behind the expanding food sensitivity pattern that so many people experience: a list of reactive foods that keeps growing, where eliminating one food leads to developing sensitivities to whatever you’re eating most frequently. The problem isn’t the foods. It’s the barrier that’s allowing those foods to activate the immune system.
Intestinal permeability is measured through zonulin in stool testing and serum LPS-binding protein. It consistently co-occurs with dysbiosis — the two conditions drive each other — which is why addressing one without the other rarely produces lasting results.

6. Bile Acid Insufficiency
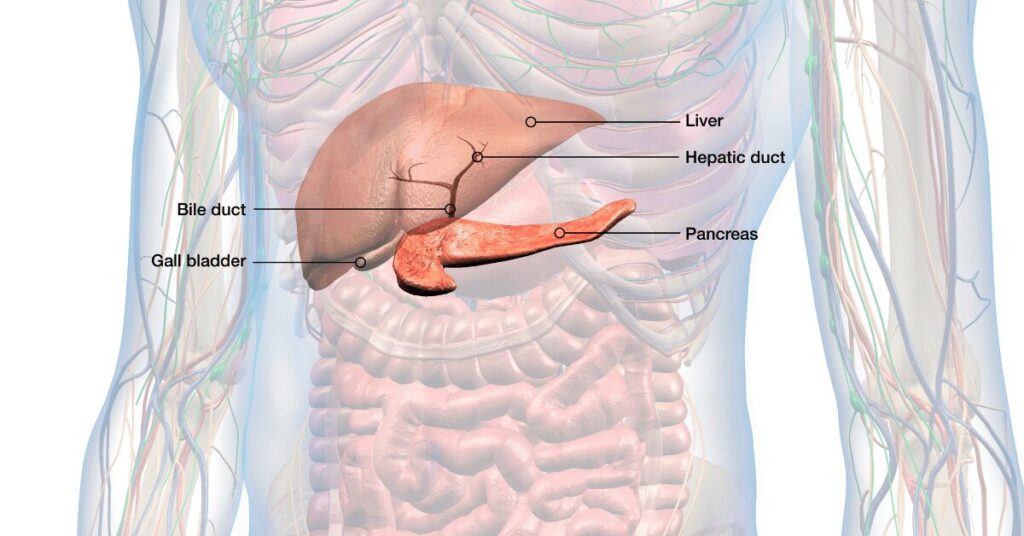
Bile is produced by the liver, stored in the gallbladder, and released into the small intestine when you eat fat. It emulsifies fat for digestion and acts as a natural antimicrobial in the small intestine — one of the mechanisms that helps keep bacterial populations in check.
When bile production is inadequate, fat digestion is impaired. Undigested fats move through the small intestine and into the colon, where bacteria ferment them — creating the gas and bloating that follows fatty meals. The bloating often comes with pale or floating stools, nausea after fatty foods, and a particular heaviness after meals.
Bile acid insufficiency is particularly common after gallbladder removal — a surgery performed on approximately 700,000 people in the US annually. The gallbladder stores concentrated bile for release in response to a fatty meal. Without it, bile drips continuously into the small intestine in dilute amounts rather than being released in an appropriate bolus. Fat digestion becomes chronically impaired.
But bile insufficiency also occurs with intact gallbladders when liver function is suboptimal, when bile acid recycling in the terminal ileum is impaired by inflammation or SIBO, or when dietary fat intake is very low and bile production is chronically suppressed.
Restoring bile flow — through bile salts, phosphatidylcholine, or bile acid support — addresses the digestion issue and the antimicrobial deficit simultaneously.
7. Histamine Intolerance
Histamine intolerance is one of the most consistently missed drivers of chronic bloating because the symptoms are so scattered and the connection to gut bacterial balance is so rarely made.
The mechanism involves two factors operating together. First, certain dysbiotic bacteria — particularly Morganella morganii and some Klebsiella species — produce histamine directly as a metabolic byproduct. When these bacteria overgrow, histamine production in the gut increases before you’ve eaten anything high in histamine.
Second, dysbiosis and gut lining damage deplete DAO — diamine oxidase — the enzyme produced by intestinal cells that breaks down histamine. When DAO is low, dietary histamine from wine, leftovers, aged cheese, fermented foods, and cured meats can’t be cleared properly and accumulates.
The result: bloating, gut cramping, skin flushing, headache, racing heart, and anxiety that appear to be random food reactions but are actually a bacterial balance and gut lining problem. The pattern is often dismissed as general food sensitivity or, when the cardiac and anxiety symptoms dominate, attributed to anxiety disorder.
Antihistamines provide temporary symptom relief but don’t address the underlying DAO deficiency or the dysbiosis producing excess histamine. The problem recurs until the gut environment is restored.

8. Estrogen Dominance and Slow Motility
The gut-hormone connection is one of the most clinically significant and least discussed drivers of bloating — particularly in people who notice that their bloating is consistently worse in the week before their period or at specific points in their cycle.
Estrogen receptors line the gut wall and directly regulate gut motility. When estrogen levels are elevated relative to progesterone — a pattern called estrogen dominance — gut transit slows. Food moves through more slowly, fermentation increases, and bloating worsens.
Estrogen dominance can occur from excess estrogen production, from impaired liver clearance of estrogen, or from disrupted estrobolome function. The estrobolome — the community of gut bacteria that metabolizes estrogen — controls how much estrogen gets deconjugated and reabsorbed versus excreted. When dysbiosis disrupts estrobolome composition and elevates beta-glucuronidase activity, estrogen recirculation increases.
This creates a bidirectional relationship: gut dysbiosis drives estrogen dominance, which slows gut motility, which worsens dysbiosis and fermentation. People with this pattern often notice that their bloating is particularly responsive to the menstrual cycle — but addressing only the hormonal side while ignoring the gut produces incomplete results, and addressing only the gut while ignoring the hormonal component does the same.

9. Hypothyroidism
Thyroid hormone directly regulates gut motility — a connection that’s well-established in the literature but consistently overlooked in practice. The relationship between thyroid function and constipation is widely known. The relationship between subclinical hypothyroidism and chronic bloating is less often made.
Thyroid hormone stimulates the smooth muscle contractions that move contents through the gastrointestinal tract. When thyroid function is reduced — even subclinically, with TSH in the “normal” range but above the functional optimal of 1 to 2 — gut transit slows. Food moves through more slowly. Bacterial fermentation has more time to accumulate. Bloating builds.
The pattern often includes constipation or infrequent bowel movements, lower abdominal bloating that’s worse by evening, and the constellation of other hypothyroid symptoms: fatigue, cold intolerance, hair thinning, brain fog, and difficulty losing weight.
Standard thyroid testing — TSH alone — misses subclinical hypothyroidism and functional hypothyroidism where TSH is normal but Free T3 (the active form of thyroid hormone) is low. This is why someone can be told their thyroid is fine while experiencing all the symptoms of insufficient thyroid hormone, including gut symptoms that don’t resolve until thyroid optimization is addressed.

10. Stress-Driven Gut Dysmotility
Chronic stress isn’t just emotionally difficult. It creates specific, measurable physiological changes in the gut that drive bloating — and those changes don’t resolve when the stressor passes if the stress has been chronic and prolonged.
Cortisol suppresses digestive enzyme production — reducing the stomach acid, pancreatic enzymes, and bile required for efficient digestion. It shifts blood flow away from the gut toward skeletal muscle, reducing the oxygen and nutrients available to intestinal cells. It directly alters gut motility through its effects on the enteric nervous system and the migrating motor complex.
The vagus nerve — the primary communication pathway between the brain and the gut — is directly affected by chronic stress. Vagal tone decreases under chronic stress conditions, impairing the parasympathetic signaling that coordinates digestion, enzyme secretion, and gut motility. A gut that isn’t receiving adequate parasympathetic input doesn’t digest efficiently, doesn’t coordinate peristalsis normally, and creates the conditions for fermentation, bloating, and dysbiosis.
This is why people who can identify a specific period of high stress as the starting point for their gut symptoms often find that the gut symptoms persist long after the stressor has resolved. The stress normalized the gut into a dysfunctional state, and the gut doesn’t spontaneously recover without addressing the vagal tone, HPA axis function, and microbial changes that accumulated during that period.
Why This List Matters
The reason this list exists — the reason there are ten distinct mechanisms rather than one — is that bloating is a symptom. A final common pathway. Multiple different physiological breakdowns can produce the same outcome: a distended, uncomfortable abdomen.
Treating “bloating” with a generic protocol makes as much sense as treating “chest pain” with a single medication regardless of whether the cause is a cardiac event, a pulled muscle, or acid reflux. The treatment needs to match the mechanism.
This is also why the same protocol that resolved someone else’s bloating — the elimination diet, the probiotic, the gut healing powder — doesn’t work for you. Their mechanism isn’t yours. Their protocol isn’t designed for your physiology.
The starting point is identifying which of these mechanisms is actually driving your pattern. Sometimes it’s one. Often it’s several operating simultaneously and feeding each other — dysbiosis driving intestinal permeability, which drives immune activation, which drives histamine intolerance, which drives bloating from multiple angles at once.
That’s why testing matters. Not to collect information for its own sake, but because the protocol that comes from knowing your specific pattern looks completely different from a generic approach — and it actually works.
→ Download the free Bloating Body Map to identify which zone your bloating pattern falls into — the first step toward understanding which of these mechanisms is most likely at play.
Ready to find out which root cause is actually driving your bloating? Complete our Digestive Health Assessment and our team will review your full symptom profile to determine your most strategic next step.
→ Start Your Digestive Health Assessment here
After reviewing your responses, we’ll recommend the right path forward — whether that includes functional gut testing, a targeted protocol, or a personalized strategy session.
Bloating is a symptom. Not a life sentence. And when you know the mechanism, you know what to address.





