You’ve done the therapy. You’ve tried the breathing exercises, the journaling, the supplements your friend swore by. Maybe you’ve been on medication that helped for a while, or helped a little, or helped at first and then stopped.
And there’s always this floor you can’t get below. A baseline hum of anxiety that responds to the work and then comes back when the work pauses—like it has its own source that nothing you’re doing is actually touching.
Here’s what nobody has told you: anxiety is not one thing.
It is a symptom with multiple possible biological drivers. And the reason most people spend years trying interventions that help a little but never quite get there is because the type was never identified. The approach that works for metabolic anxiety is not the approach that works for hormonal anxiety. The intervention for HPA-axis dysregulation is not the intervention for neuroinflammation.
If the type is wrong, the treatment is wrong—even if it’s the right treatment for someone else with the same diagnosis.
Here are the four types I see most often in practice, what distinguishes them, and what the biology actually looks like underneath each one.
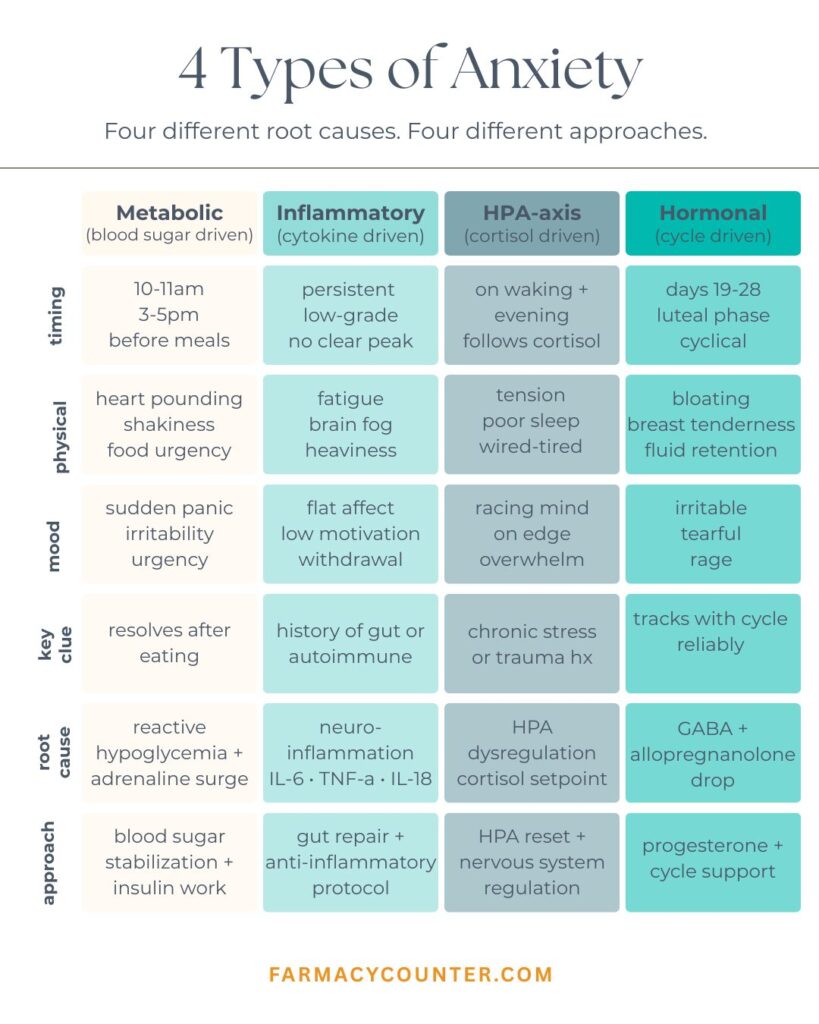
Type 1: Metabolic Anxiety
The pattern: Worst before meals, mid-morning around 10 or 11am, and mid-to-late afternoon. Comes with physical symptoms—heart pounding, shakiness, sudden urgency around food, difficulty concentrating until you eat. Often misidentified as generalized anxiety disorder or panic disorder because the physiological experience is essentially identical.
The mechanism: The root of metabolic anxiety is reactive hypoglycemia and blood sugar instability. When blood glucose drops, the body releases adrenaline (epinephrine) as a counter-regulatory hormone to signal the liver to release stored glucose and restore blood sugar levels. This is a normal and protective response.
The problem is that the physiological experience of an adrenaline surge—racing heart, shakiness, sweating, a sense of urgency or dread—is indistinguishable from anxiety. The nervous system doesn’t categorize it differently. An adrenaline release triggered by a blood sugar drop feels exactly like an adrenaline release triggered by a perceived threat.
For people with reactive hypoglycemia, this happens multiple times daily on a predictable schedule. The body oscillates between blood sugar spikes (often from carbohydrate-heavy meals or snacks) and rapid drops, triggering adrenaline each time glucose falls. The anxiety follows this pattern precisely, which is the diagnostic clue most practitioners miss because they’re not asking about the timing relative to food intake.
What makes it distinctive: The timing is the tell. Anxiety that arrives predictably at 10am, 3pm, or right before dinner is following a physiological pattern, not an emotional one. If eating something reliably stops the anxiety, if skipping a meal reliably triggers it, if you feel fine after meals and unwell a few hours later—that is a metabolic signal, not a psychological one.
What standard care misses: Blood sugar is almost never assessed in the context of anxiety treatment. No one asks whether symptoms correlate with meal timing. No one checks fasting insulin or runs a glucose tolerance test. The patient gets an anxiety diagnosis and a prescription, and their blood sugar keeps doing exactly what it was doing before.

Type 2: Inflammatory Anxiety
The pattern: More diffuse and harder to pin to a specific time of day. Accompanied by brain fog, physical fatigue, low motivation, and a flat or heavy mood that sits underneath the anxiety. Often co-presents with a history of gut issues, autoimmune conditions, skin problems, or chronic infections. May feel worse after eating certain foods, when sick, or during high-stress periods.
The mechanism: The inflammatory theory of mood disorders is one of the most robust findings in modern neuroscience, and yet it is almost never part of how anxiety is assessed or treated.
When inflammation is present anywhere in the body, inflammatory cytokines—specifically IL-1β, IL-6, and TNF-alpha—circulate through the bloodstream. These cytokines cross the blood-brain barrier, particularly when that barrier is already compromised by chronic inflammation (which it often is). Once in the brain, they activate microglia, the brain’s resident immune cells.
Chronically activated microglia produce their own inflammatory mediators, which directly disrupt neurotransmitter synthesis and receptor function. The most clinically significant pathway is what happens to tryptophan. Inflammation activates an enzyme called IDO (indoleamine 2,3-dioxygenase), which shunts tryptophan away from serotonin production and toward the production of kynurenine pathway metabolites—including quinolinic acid, a potent neurotoxin that overstimulates NMDA receptors, creates oxidative stress, and impairs neuronal function (1).
The result is anxiety and depression that doesn’t respond to serotonin-targeting medications—because the problem isn’t serotonin reuptake. The problem is that serotonin isn’t being produced in the first place. You can’t reuptake what isn’t there.
What makes it distinctive: Inflammatory anxiety tends to be diffuse rather than episodic. It doesn’t follow a clock. It doesn’t respond predictably to eating or not eating. It often comes with a heaviness or flatness alongside the anxiety—not just nervousness, but exhaustion and fog layered on top of it. The history is often revealing: gut dysbiosis, food sensitivities, autoimmune conditions, a chronic infection that never fully resolved, or an acute illness or significant stressor that preceded the onset of anxiety symptoms.
What standard care misses: The majority of people treated for depression and anxiety have never had their inflammation measured. hs-CRP, IL-6, and ferritin are not part of any standard psychiatric workup. Neuroinflammation doesn’t show up on an MRI. It doesn’t show up in a basic metabolic panel. It is completely invisible to standard care, which means the mechanism driving the anxiety is never identified and never addressed.

Type 3: HPA-Axis Anxiety
The pattern: Follows the cortisol curve. Worst in the morning—often waking with a racing mind, a sense of dread before anything has happened, or an inability to settle into the day. May include a second peak of anxiety in the evening, with wired-but-tired insomnia: exhausted but unable to fall asleep, mentally activated even when physically depleted. Often accompanied by poor stress tolerance, easy overwhelm, and a sense that everything requires more effort than it should.
The mechanism: The hypothalamic-pituitary-adrenal (HPA) axis is the body’s central stress response system. The hypothalamus signals the pituitary, which signals the adrenal glands to release cortisol. In a healthy, well-regulated system, cortisol peaks in the early morning, gradually declines through the day, and reaches its lowest point at night—the circadian cortisol rhythm that allows for restful sleep and morning alertness.
When the HPA axis is dysregulated—from chronic stress, poor sleep, or a history of acute stress events that alter the setpoint of the stress response—this rhythm breaks down. The curve can be flattened, inverted, elevated across the board, or erratic. In any of these patterns, the nervous system is receiving incorrect signals about the level of threat in the environment.
An elevated morning cortisol curve produces the experience of waking already in a state of activation—mind already racing, already anticipating problems, already in mild threat response before the day begins. An elevated evening curve prevents the wind-down that normal cortisol decline produces, creating the wired-but-tired state where the body is exhausted but the nervous system won’t quiet.
Cortisol also directly modulates GABA receptor sensitivity and interacts with serotonin synthesis. A dysregulated cortisol curve isn’t just creating subjective stress—it’s biochemically altering the neurotransmitter environment in ways that produce anxiety at the receptor level (2).
What makes it distinctive: The timing pattern relative to the cortisol curve is the key diagnostic feature. Morning anxiety that exists before any stressor has occurred, that begins improving as the day progresses, points toward an elevated morning cortisol. Wired-but-tired evenings with racing thoughts that prevent sleep point toward a secondary cortisol peak that should have resolved. The pattern responds to—and is worsened by—sleep quality, which directly affects HPA axis regulation.
What standard care misses: Cortisol rhythm is not tested in standard anxiety care. A single morning cortisol measurement tells you almost nothing about the full curve. DUTCH testing or four-point salivary cortisol gives you the complete picture—the arc of cortisol through the day and evening, the cortisol awakening response, and the metabolites that tell you how cortisol is being cleared. None of this is part of conventional psychiatric assessment.

Type 4: Hormonal Anxiety
The pattern: Cyclical and predictable in premenopausal women. Intensifies in the luteal phase—the 7 to 10 days before menstruation—and often improves within a day or two of the period starting. At perimenopause, may shift from cyclical to more persistent, often worsening alongside other hormonal transition symptoms. The hormonal-anxiety connection is so strong that many women can predict their worst anxiety days by their cycle calendar.
The mechanism: Estrogen and progesterone both have direct effects on the neurochemistry that regulates anxiety, and when they fluctuate or decline, those neurochemical effects fluctuate and decline with them.
Estrogen does three things that are directly relevant to anxiety. It upregulates serotonin receptor density—particularly 5-HT2A receptors. It supports serotonin transporter expression. And it modulates the HPA axis, helping regulate the cortisol response to stress. When estrogen drops in the late luteal phase or at perimenopause, all three of these regulatory effects drop with it.
Progesterone’s effect on anxiety operates through a different pathway. In the brain, progesterone is converted to a neurosteroid called allopregnanolone. Allopregnanolone is one of the most potent positive modulators of the GABA-A receptor in the body—the same receptor targeted by benzodiazepines. It binds GABA-A receptors and produces calming, anti-anxiety, sedating effects. Think of it as the body’s endogenous Valium.
When progesterone drops in the late luteal phase—which it does, sharply—allopregnanolone drops with it. GABA signaling drops. The nervous system loses one of its primary calming mechanisms at exactly the point in the cycle when estrogen-based serotonin support is also declining. The combined neurochemical effect of losing both estrogen-serotonin support and progesterone-GABA support simultaneously maps directly onto anxiety, irritability, sleep disruption, and emotional fragility (3).
At perimenopause, this isn’t cyclical anymore. As progesterone declines ahead of estrogen and both become erratic, the neurochemical environment becomes unpredictable. Anxiety that was previously premenstrual becomes persistent. Sleep becomes unreliable. Emotional regulation becomes effortful in a way it never was before.
What makes it distinctive: The cyclical pattern is the signature. Anxiety that is reliably worse in the 7 to 10 days before menstruation and reliably better once the period starts is hormonal anxiety until proven otherwise. The predictability is diagnostic—psychological anxiety doesn’t follow a 28-day calendar. At perimenopause, onset or worsening of anxiety that coincides with the beginning of cycle irregularity is the clinical signal.
What standard care misses: Hormonal workups in the context of anxiety are almost never done. A standard psychiatric evaluation doesn’t include a comprehensive hormone panel, doesn’t assess progesterone-to-allopregnanolone conversion, and doesn’t look at the relationship between symptom timing and the menstrual cycle. Women with premenstrual or perimenopausal anxiety are often given antidepressants with no investigation into the hormonal mechanism driving their symptoms.

Why Most People Have More Than One Type
In practice, most patients present with more than one type running simultaneously. The investigation tells us which is dominant and where to start—but it rarely tells a single-driver story.
Metabolic dysfunction drives inflammation: blood sugar instability causes cortisol spikes, which create oxidative stress, which promotes neuroinflammation. Neuroinflammation dysregulates the HPA axis: chronically elevated inflammatory cytokines directly alter the hypothalamic setpoint of the stress response. HPA-axis dysregulation depletes the hormonal environment: chronically elevated cortisol suppresses progesterone production, directly worsening hormonal anxiety.
These systems are not separate. They communicate constantly, and dysfunction in one propagates dysfunction in others. This is why anxiety can feel so complex and so resistant to interventions that address only one component. You clean up the gut, and it helps some. You support adrenals, and it helps some. But the picture doesn’t resolve because the other drivers are still active.
This is also why the type matters so much. Starting with the primary driver—the one that started the cascade—changes the outcome significantly. Addressing secondary drivers without identifying the primary one often produces partial improvement that doesn’t hold.
What Actually Needs to Be Assessed
When someone comes to me for anxiety that hasn’t responded adequately to what they’ve already tried, I’m not starting with a symptom questionnaire. I’m starting with an investigation into the biology.
For metabolic anxiety, I’m looking at fasting glucose, fasting insulin, and HbA1c to assess blood sugar regulation baseline. In some cases, a glucose tolerance test with insulin levels gives more granular information about reactive patterns.
For inflammatory anxiety, I’m looking at hs-CRP, ferritin, IL-6, homocysteine, and comprehensive stool analysis to identify the source of inflammation—whether it’s gut-driven, immune-driven, or metabolic. I’m looking at the kynurenine pathway through organic acids testing, which shows whether tryptophan is being shunted away from serotonin and toward neurotoxic metabolites.
For HPA-axis anxiety, I’m running a DUTCH test—a comprehensive dried urine panel that gives me the full cortisol curve across the day, the cortisol awakening response, cortisol metabolites, and the sex hormone picture that interacts with HPA function. A single morning cortisol tells me almost nothing about the actual rhythm.
For hormonal anxiety, I’m looking at the full hormone picture at the right point in the cycle: estradiol, progesterone, LH, FSH, and DHEA-S in premenopausal women, with particular attention to progesterone levels in the mid-luteal phase, which is when allopregnanolone should be at its peak. In perimenopausal women, the pattern over time matters more than any single measurement.
Across all types, I’m also looking at the methylation status—homocysteine, MTHFR variants, whole blood histamine—because methylation is required for neurotransmitter synthesis, and impaired methylation capacity amplifies whatever anxiety type is present. I’m looking at the full thyroid panel including free T3 and reverse T3, because thyroid function affects every biological system involved in anxiety and is almost always assessed incompletely in standard care.
How the Approach Changes by Type
This is why type identification matters clinically. The intervention for one type can be actively unhelpful for another.
For metabolic anxiety, the foundation is blood sugar stabilization: protein and fat at every meal, reduced refined carbohydrate load, consistent meal timing, and addressing insulin resistance if present. Supplementation with chromium, berberine, or inositol may be appropriate depending on the picture. None of these interventions address inflammatory anxiety.
For inflammatory anxiety, the work is identifying and removing the inflammatory driver—gut dysbiosis, food sensitivities, chronic infection, environmental triggers—and using targeted anti-inflammatory support (omega-3 fatty acids, curcumin, specialized pro-resolving mediators) while the gut-brain axis is repaired. Without addressing the source of inflammation, neurotransmitter precursors like 5-HTP have limited effect because the tryptophan pathway is being shunted away from serotonin regardless of what you supplement.
For HPA-axis anxiety, the HPA setpoint needs to be recalibrated through consistent sleep architecture, cortisol rhythm support, and targeted adaptogenic support depending on whether cortisol is elevated or depleted. In many cases, addressing the sleep disruption that perpetuates HPA dysregulation is the most important intervention. Stimulatory approaches that work for other anxiety types can significantly worsen HPA-axis anxiety.
For hormonal anxiety, the approach depends on where in the hormonal picture the disruption sits. Supporting progesterone-to-allopregnanolone conversion, addressing estrogen metabolism, and in perimenopausal women, considering bioidentical hormone support—all require knowing what the actual hormone levels and metabolites are doing, not guessing based on symptoms alone.

Why Conventional Approaches Miss This
Anxiety has a diagnosis. The diagnosis leads to a treatment category. The treatment category is applied uniformly regardless of biology.
This approach isn’t designed to identify type. It isn’t designed to ask why anxiety is present at the biological level. It’s designed to reduce symptoms through a standardized intervention—which is why so many people experience partial response, or initial response that fades, or no response at all. The intervention doesn’t match the mechanism.
The reason so many people spend years trying interventions that help a little but never get them all the way there is not that they’re doing something wrong, or that their anxiety is untreatable, or that they need to work harder on stress management. It’s that the type was never identified, so the approach was never calibrated to their actual biology.
What Happens When the Type Is Correctly Identified
When the right type is identified and the protocol is built from that foundation, the results are different in kind, not just degree.
Metabolic anxiety that has been mismanaged as generalized anxiety for years often shows rapid improvement—sometimes dramatic—within the first few weeks of blood sugar stabilization, because the underlying mechanism responds quickly to the correct intervention.
Inflammatory anxiety that has been treated with serotonin-targeting medication without addressing the inflammatory driver often shows limited response to medication and significant improvement when the gut-brain axis is repaired, because now tryptophan can actually be used to build serotonin.
HPA-axis anxiety that has been treated with stimulants or high-dose caffeine—which many people use to cope with the fatigue it creates—often worsens under those interventions and shows significant improvement when the cortisol rhythm is properly assessed and addressed.
Hormonal anxiety that has been treated as generalized anxiety without any hormonal workup often shows dramatic improvement when the progesterone-allopregnanolone pathway is supported—sometimes with targeted supplementation, sometimes with bioidentical support, depending on the clinical picture.
The biology is findable. When it’s found, the approach changes. When the approach changes, the results change.
Let’s Identify Your Type
If you’re recognizing your pattern in one or more of these descriptions, the Anxiety Pattern Decoder is the clearest starting point. It walks you through the four biological types, includes a short assessment to identify which one is most likely dominant for you, and explains what your result means for how to actually address it.
Download it free below.
References:
- Dantzer R, O’Connor JC, Freund GG, Johnson RW, Kelley KW. From inflammation to sickness and depression: when the immune system subjugates the brain. Nat Rev Neurosci. 2008;9(1):46-56. doi:10.1038/nrn2297
- Tsigos C, Kyrou I, Kassi E, Chrousos GP. Stress: Endocrine Physiology and Pathophysiology. In: Endotext. MDText.com, Inc.; 2020. Updated October 17, 2020.
- Bäckström T, Bixo M, Johansson M, et al. Allopregnanolone and mood disorders. Prog Neurobiol. 2014;113:88-94. doi:10.1016/j.pneurobio.2013.07.005





